MEGALOBLASTIC ANAEMIA- simple way to prevention
Definition
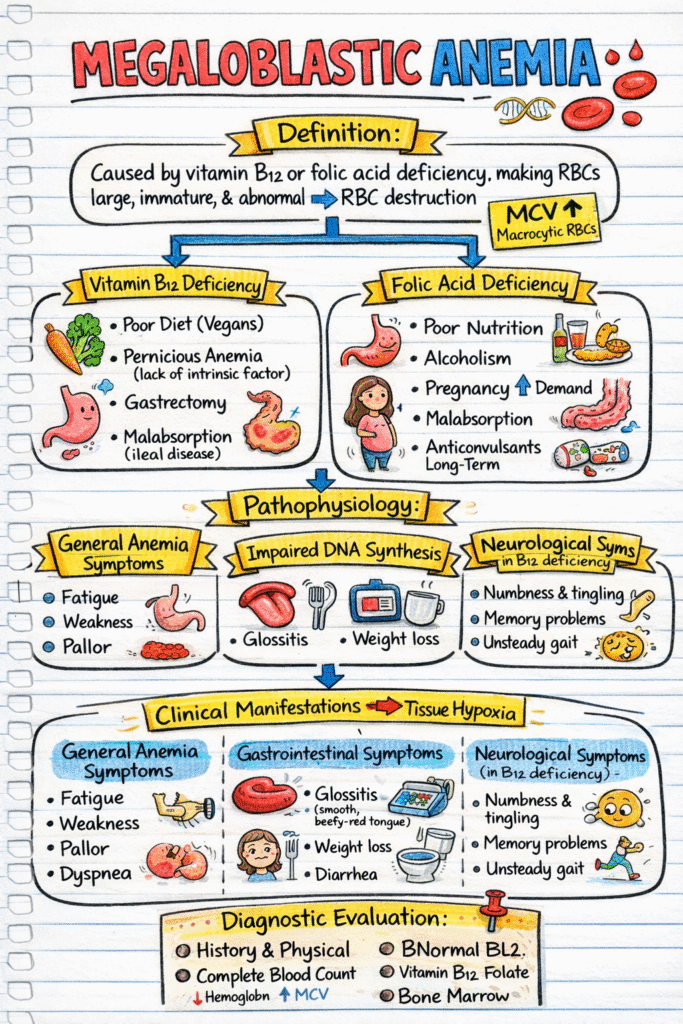
Megaloblastic Anaemia is caused by vitamin B12 or folic acid deficiency which makes RBCs to large, immature, and abnormal which leads to RBCs destruction.
Megaloblastic anaemia is a condition in which the red blood cells become larger than normal. Anaemia itself means that the blood does not have enough healthy red blood cells to supply adequate oxygen to the body.
In this type of anaemia, the problem occurs during the formation of red blood cells in the bone marrow. The cells are unable to make DNA properly, which is necessary for normal cell division. Because of this, the cells keep growing but do not divide as they should. As a result, large and immature red blood cells are produced.
Megaloblastic anaemia usually develops gradually, so symptoms may appear slowly over time rather than suddenly.
The most common reason for this condition is a lack of important vitamins, especially vitamin B12 or folic acid. These vitamins are essential for DNA production. When the body does not get enough of them, or cannot absorb them properly, normal red blood cell formation is disrupted, leading to megaloblastic anaemia.
Basic Anatomy & Physiology
Normal RBC Formation:
- DNA synthesis needed for cell division
- Requires vitamin B12 & folic acid
In Megaloblastic Anaemia:
- DNA synthesis impaired
- Cells grow but don’t divide properly
- RBCs become macrocytic
NOTE- MCV ↑ (macrocytic anaemia)
Causes of Megaloblastic Anaemia
1. Vitamin B12 Deficiency
Causes:
- Poor dietary intake (vegans)
- Pernicious anaemia (lack of intrinsic factor)
- Gastrectomy
- Malabsorption (ileal disease)
2. Folic Acid Deficiency
Causes:
- Poor diet
- Alcoholism
- Pregnancy
- Malabsorption
- Long-term anticonvulsant use
Remember- Giving folic acid alone in B12 deficiency improves anaemia but worsens nerve damage
Pathophysiology
Deficiency of vitamin B₁₂ and/or folic acid
↓
Inadequate intake / Poor absorption / Increased requirement / Drug interference
↓
Reduced availability of vitamin B₁₂ or folate in the body
↓
Impaired DNA synthesis in bone marrow cells
↓
Defective nuclear maturation of red blood cell precursors
↓
Normal cytoplasmic maturation but delayed nuclear division
↓
Formation of large, immature red blood cells (megaloblasts)
↓
Ineffective erythropoiesis in bone marrow
↓
Premature destruction of abnormal red blood cells
↓
Reduced number of mature red blood cells in circulation
↓
Decreased oxygen-carrying capacity of blood
↓
Tissue hypoxia
Clinical Manifestations
General Anaemia Symptoms
- Fatigue
- Weakness
- Pallor
- Dyspnoea
Gastrointestinal Symptoms
- Glossitis (smooth beefy-red tongue)
- Loss of appetite
- Weight loss
- Diarrhoea
Neurological Symptoms (ONLY in B12 deficiency)
- Numbness & tingling
- Memory problems
- Unsteady gait
- Confusion
Remember- Anaemia + neurological symptoms = vitamin B12 deficiency
Diagnostic Evaluation
1. History and physical examination
2. Complete Blood Count (CBC)
- ↓ Haemoglobin
- ↑ MCV
3. Peripheral Blood Smear
- Large oval RBCs
- Hyper segmented neutrophils
4. Vitamin Levels
- ↓ Serum B12
- ↓ Serum folate
5. Bone Marrow (rarely needed)
- Megaloblasts present
Medical Management
1. Vitamin B12 Deficiency-
- IM vitamin B12 injections (especially if malabsorption)
Note- Often lifelong therapy in pernicious anaemia
2. Folic Acid Deficiency
- Oral folic acid
Note– Always rule out B12 deficiency before giving folate alone.
Dietary Management
1. Vitamin B12-Rich Foods
- Meat
- Fish
- Eggs
- Milk
2. Folic Acid-Rich Foods
- Green leafy vegetables
- Citrus fruits
- Beans
- Whole grains
Note- Alcohol decrease the folate absorption
Nursing Care Plan (NCP) –
1. NCP 1: Fatigue
Related to: Decreased oxygen delivery
Evidenced by: Weakness, lethargy
Interventions:
- Plan rest periods
- Assist with ADLs
- Monitor Hb levels
2. NCP 2: Impaired Physical Mobility (B12 deficiency)
Related to: Neurological impairment
Interventions:
- Fall precautions
- Assist ambulation
- Assess sensation & gait
Evidence: Prevents injury due to neuropathy.
3. NCP 3: Imbalanced Nutrition
Related to: Vitamin deficiency
Interventions:
- Diet education
- Encourage vitamin-rich foods
- Refer to dietitian
4. NCP 4: Risk for Injury
Related to: Neuropathy & confusion
Interventions:
- Safe environment
- Frequent orientation
- Bed in low position